I’ve been working in the food allergy world for over ten years. It is not an “industry” I would have chosen, food allergies choose you. But one of the silver linings is the people that are in this work, the love, the intelligence and the profound commitment. There are parents with phenomenal backgrounds: finance, accounting, legal and so much more. So when my friend, Lianne, reached out this morning and asked if we could share her new article, we did not hesitate. We are so much strong together. Please share this with others, so that together, we can protect the health of the 1 in 13 children that now has food allergies in America.
“It was a blustery Sunday morning about 2 years ago; one of those days you can justify sitting at home and going through your Facebook feed. I typed “nut allergy” into the search bar to see if any interesting posts would turn up. That morning, a post did catch my attention. It was on an online motherhood support page that discussed wide ranging issues from breast-feeding to family friendly restaurants in New York City. The site had almost over 200,000 followers.
The post detailed a story of a young new mom, let’s call her Pam, who went to the park with her 2 year old. Once there, she took out her child’s lunch, a peanut butter sandwich. Pam’s child, being a 2 year old, naturally had sticky fingers after eating, which was noticed by another mom (lets call her Sue), nearby. Sue had a child with a peanut allergy and looking very panicked asked Pam to please wash her daughter’s hands before going back on the playground. The post was a rant on Pam’s response to being asked to wash her child’s hands by peanut allergic mom Sue. Pam cursed Sue online, told her this was an f”ing public space and that she and her precious snowflake would not be dictating policy. This was not what caught my attention; however, it was the comments from a multitude of other moms (too many to count) agreeing in the most vicious way. The supporting comments were downright mean, some even wishing actual harm to an innocent two-year-old child. I was shocked that other moms on a parenting support site would say such things directed at someone’s child.
I often think of this post when I advocate for consistent policies for passengers with food allergies on planes. There are many people out there who do not understand the potential severity of food allergies and many of them are potential passengers on planes. As a community, in order to affect meaningful change in the air and other venues, we must support and love each other because the outside world is sometimes a very unfriendly and uneducated space. When we publicly disparage one another in the food allergy space because we feel a fellow parent is doing something alarmist or different than we would, we do not serve our community well. Let me use the mom on the playground to illustrate my point.
I realize it is not realistic that peanut allergic mom Sue can police what other children are eating in a public space. This is not a classroom or a situation where you are up in the air with nowhere to go and she can just leave if she is uncomfortable with peanut butter in the area. I can easily see in the current combative food allergy Facebook climate, with many other food allergy moms chiming in, telling Sue she is being paranoid, rude or perhaps that other food allergies are just as dangerous as peanuts and why not ban all food on the playground with her attitude. We need to be a bit more introspective and compassionate to each other, if we are trying to educate those outsiders around us to be kind to our children.
Perhaps Sue’s child is newly diagnosed and it’s the first time she ventured out to the playground and she panicked when she saw the peanut butter? Maybe her child reacted to a small amount and she had recently been in the hospital for anaphylaxis. Maybe she is just frightened and nervous. I don’t know what was going through Sue’s mind but I do know she is a fellow food allergy mom and she is scared. This is the person whom we need to nurture and support on and offline, not condemn or criticize. Everyone’s life experiences are different and so is their choice on how to manage their child’s food allergy. If your child had an airborne reaction, you may have a very different management plan. We can never be in someone else’s shoes even with the same diagnosis and we must NOT level judgment that is mean spirited at each other in our own community. If someone is brave enough to post his or her experience, start a petition for change or initiate a lawsuit, we must realize that this does take courage. If you don’t agree, scroll on by, don’t add your signature, or post something helpful like a medical study to allay that person’s fears, but it is my humble opinion that we do the community as a whole damage when we cut each other down using derisive language.
One of my mentors, Robyn O’Brien, constantly speaks about bringing change by using love. She is a shining example of this idea working. We could all show a little more love to our fellow food allergy moms. That does not mean we don’t disagree; indeed great change can be achieved by a healthy debate. We must realize that food allergies are not a competition about which strategy is correct, which advocacy group is best, or which treatment is right. Everyone in this space is trying in their own best way to help those who live with life threatening allergies. If we want others outside our community to respect our life threatening food allergies, we must respect and learn from each other inside our food allergic world as well.”
Truth: No thorough allergenicity assessment is conducted on GMO foods
[/vc_column_text][vc_empty_space height=”10px”][vc_row_inner css=”.vc_custom_1467578094543{margin-right: 0px !important;margin-left: 0px !important;}”][vc_column_inner width=”1/2″][vc_column_text]Most food allergies are caused by a reaction to a protein in a food. The DNA of an organism contains instructions for making proteins. Genetic engineering changes the DNA of a food, and the altered DNA can in turn create new proteins. GM foods could create new allergies in two ways: the new proteins could cause allergic reactions (be allergens) themselves, or the new proteins could sensitize people to existing food proteins.
The website GMO Compass, which is run by the public relations firm Genius GmbH, claims that GM plants pose no greater risk than new varieties of crops obtained through conventional breeding, or the importation of new exotic foods, which can also result in new allergens appearing in the diet.1
But independent scientists disagree. A 2003 review states that compared with conventional breeding, GM has a “greater potential to introduce novel proteins into the food supply” and increase the likelihood of allergic reactions.2[/vc_column_text][vc_empty_space height=”10px”][/vc_column_inner][vc_column_inner width=”1/2″][vc_column_text css=”.vc_custom_1453588389435{padding-top: 20px !important;padding-right: 20px !important;padding-bottom: 20px !important;padding-left: 20px !important;background-color: #eaeaea !important;}”]
Myth at a glance
The public is told that GM foods are no more likely to cause allergic reactions than non-GM foods and that they are fully assessed for allergenicity. But this is untrue. Genetic engineering can create novel proteins that have no history of safe use in food, raising the potential for allergic reactions.
The absence of reliable methods for allergenicity testing and the lack of rigour in current allergy assessments mean that it is impossible to reliably predict whether a GMO will prove to be allergenic.
If a GMO did prove to be allergenic, it would be almost impossible to find out, as no post-commercialization monitoring is carried out anywhere in the world.
[/vc_column_text][/vc_column_inner][/vc_row_inner][/vc_column][/vc_row][vc_row][vc_column][vc_row_inner][vc_column_inner][vc_empty_space height=”10px”][/vc_column_inner][/vc_row_inner][vc_column_text]A study on humans confirmed the potential for GM to create novel and potentially allergenic proteins. One of the experimental subjects showed an immune response to GM soy but not to non-GM soy. GM soy was found to contain at least one protein that was different from the profile of proteins present in the non-GM variety.3 The study did not show that GM soy is more allergenic than non-GM soy, but it did show that a GM food can unexpectedly cause an allergic reaction in a person who is not allergic to the food in its non-GM form.
The EU system for assessing GM foods for allergenicity
Under European law, GM foods must be assessed for their potential to cause allergies before they are allowed onto the market. Proponents claim that any potentially allergenic GM foods are likely to be caught by these regulatory checks. The GMO Compass website calls these assessments “rigorous” and adds, “If a GM plant is found to contain a potential allergen, its chances of receiving approval in the EU are slim to none.”1
But in reality, the European regulatory process, though stronger than the US process, has no rigorous system for assessing the allergenic potential of GM foods. This is largely because reliable scientific tests to predict allergenicity have not been developed.
The process that EU regulators use to assess the allergenicity of GM foods1,4 is based on a system proposed in 2001 by the Food and Agriculture Organization (FAO) of the United Nations and the World Health Organization (WHO). This system was actually designed by two GM industry-funded groups, the International Life Sciences Institute (ILSI) and the International Food Biotechnology Council (IFBC), as the FAO/WHO freely states.5
The process begins with a comparison of the protein that the GM plant is designed to produce with known allergenic proteins. Depending on the outcome of this initial assessment, further investigations can include:
Tests to see if the new protein reacts with the blood serum of sensitive individuals
Artificial stomach tests to see if the protein is broken down easily. If it is, it is thought unlikely to be an allergen
Animal feeding trials.1
Why the allergy assessment process is ineffective
The EU’s allergy assessment is unlikely to reliably predict whether a GM food will cause allergic reactions.
The most important reason is that the new protein that is assessed in the regulatory process is normally not the protein as expressed in the whole GM plant. Instead, it is what is known as a surrogate protein. This surrogate protein is isolated from sources such as GM E. coli bacteria or occasionally, a different plant species.6 This is scientifically unjustifiable because the protein can change as a result of the genetic engineering process and according to the organism within which it is expressed – as in the case of StarLink maize (Myth 3.7).
In other words, the same GM gene introduced into a GM plant and into E. coli bacteria can produce proteins that can have very different effects on the people and animals that eat them. Plants and bacteria process newly synthesized proteins in different ways. In particular, the GM plant protein will undergo a process known as “post-translational modification” and will thus possess added sugar molecules (“glycosylation”). So even though the amino acid sequences of the GM plant and GM E. coli proteins may be identical, their functions and allergenic potential can be quite different.
Other reasons why the allergenicity decision tree model is unsatisfactory include:
A comparison of the new protein in the GM food with the database of known allergens will not detect new allergens.
Blood serum tests are problematic because allergenic sensitization is an allergen-specific process. So unless the transgenic protein expressed in the GM food is already a common allergen, there is unlikely to be a single sensitized person in the world whose blood serum would react with it.2
Blood serum tests are not useful in detecting uncommon allergens – substances that few people are allergic to2 – since it is unlikely that serum samples will be taken from these few people.
A phenomenon known as cross-reactivity can make it difficult to identify from blood serum testing which specific protein out of several is the allergen.2
The artificial stomach tests carried out for regulatory purposes are performed under unrealistic conditions. Levels of acidity and digestive enzymes are much higher than would be present in the digestive systems of individuals who would consume the GM food. This makes it likely that the new GM protein will be broken down into fragments that are too small to be potent allergens. In real life, however, the levels of acidity and digestive enzymes in people’s stomachs vary according to age, health status, length of time since they ate their last meal, and other factors. One study found that under the standard conditions used in artificial stomach tests, one of the insecticidal proteins commonly present in GM Bt crops was broken down. But when the researchers adjusted the acidity and enzymes to more realistic levels, the insecticidal protein was highly resistant to being broken down. The authors called for regulatory tests to be carried out in “more physiologically relevant” conditions of lower acidity and enzyme levels.7
One review concluded that the allergenicity assessment might be useful in assessing GM foods containing a known allergenic protein, but that assessing proteins of unknown allergenicity is “more problematic” and “the predictive value of such an assessment is unknown”.2 Another review agreed that the standard tests were “not always conclusive”, especially when the organism from which the GM gene is taken has no history of dietary use or has unknown allergenicity.8
The current allergy assessment system is not reliable because it relies heavily on in vitro tests (laboratory experiments in non-living systems, such as the blood serum and artificial stomach tests). Unfortunately, however, an effective alternative does not yet exist. In vivo tests (tests on living organisms such as animals or humans) are useful for detecting nutritional or toxicological effects of foods, but no reliable animal testing methods have yet been established for allergenicity testing of foods.9,2,8,10
The main problem is that the immune systems of humans and animals are different, so it is difficult to predict human allergenicity from animal responses. The most reliable assessment of allergenicity of a GM food would be to test the food prior to commercialization, on large numbers (around 5,000) of human volunteers. The large numbers avoid false negative results (where an allergenic effect exists but is missed because too few subjects are used) and provide statistical power.
In the absence of pre-market tests on humans, at present the only reliable approach to assessing the allergenicity of GMOs would be post-commercialization monitoring. Consumers would have to be clearly informed when they ate the new GMO and would be asked to report any adverse effects to designated authorities.
Such post-commercialization assessments are not required in any country. In countries such as the US and Canada, where GM foods are not labelled, the likelihood that allergenicity would be linked to a GMO is extremely low, unless it caused acute allergic reactions in a large portion of the population.
“There is more than a casual association between GM foods and adverse health effects. There is causation as defined by Hill’s Criteria in the areas of strength of association, consistency, specificity, biological gradient, and biological plausibility.The strength of association and consistency between GM foods and disease is confirmed in several animal studies… Multiple animal studies show significant immune dysregulation, including upregulation of cytokines [protein molecules involved in immune responses] associated with asthma, allergy, and inflammation.”
– American Academy of Environmental Medicine11
Studies on GM foods confirm existing allergy assessments are inadequate
Studies on GM foods confirm that current allergy assessments are inadequate to detect new allergens created by the genetic engineering process.
In a study on mice fed GM peas containing an insecticidal protein from beans, mice showed antibody immune reactions and allergic-type inflammatory responses to the GM protein and chicken egg white protein when it was fed to them with the GM peas.12
The mice did not show antibody immune reactions and allergic-type inflammatory responses to beans that naturally contain the insecticidal protein or to egg white protein when it was fed with the natural insecticidal protein obtained from beans. They also did not have an immune response to the egg white protein when it was fed on its own.12
These outcomes show that the GM insecticidal protein made the mice more susceptible to developing allergic-type inflammatory reactions to foods eaten with the GM food. This is called immunological cross-priming.
The results indicated that the reaction of the mice to the GM peas was caused by changes brought about by the genetic engineering process. The normally non-immunogenic and non-allergenic insecticidal protein naturally produced in beans was altered in structure and/or function when engineered into peas, in particular in the addition to the protein of sugar molecules (glycosylation) via post-translational modification processes, becoming a potent immunogen (substance that produces an immune response) and allergen.12
This was not a regulatory test and tests such as this are not required to be carried out for the regulatory assessment of GM foods. The allergenicity of the GM peas would likely not have been spotted by the EU’s screening process because the natural, non-GM version of the bean insecticidal protein is not a known allergen. Because of this, blood serum from sensitized individuals would not have been available for regulatory serum tests.
Overall, the study shows that GM foods can contain new allergens and cause new allergic reactions – and that the GMO’s allergenicity is unlikely to be detected using the current allergy assessment process.
Other studies confirm the inadequacy of the current allergy assessment process:
A study on a commercialized GM insecticidal maize, MON810, showed that the GM plant’s proteins were markedly altered compared with those in the non-GM counterpart. Unexpected changes included the appearance of a new form of the protein zein, a known allergen, which was not present in the non-GM maize variety. A number of other proteins were present in both their natural forms and in truncated and lower molecular mass forms.13 These findings suggest major disruptions in gene structure and function in this GM crop. The EU’s allergy assessment failed to pick up these changes and failed to detect the presence of the newly created allergen.
A GM soy variety modified with a gene from Brazil nuts was found to be capable of producing an allergic reaction in people who are allergic to Brazil nuts. The researchers had genetically engineered the Brazil nut gene into the soy in order to increase its nutritional value. When they tested the effect of this GM soy on blood serum from people allergic to Brazil nuts, they found that the serum produced an allergic response to the soy. Through scratch tests on skin, they confirmed that people allergic to Brazil nuts were allergic to the modified soybean.14 This study is often cited by GM proponents as evidence of the effectiveness of regulatory processes in identifying allergenic foods before they reach the marketplace. But this is untrue. As with the GM peas study,12 this was not a regulatory test and tests such as this are not required to be carried out for the regulatory assessment of GM foods in any country.
Conclusion
The absence of reliable methods for allergenicity testing and the lack of rigour in current allergy assessments mean that it is impossible to reliably predict whether a GMO will prove to be allergenic. If a GMO did prove to be allergenic, it would be almost impossible to find out, as no post-commercialization monitoring is carried out anywhere in the world.
References:
GMO Compass. The allergy check. 2006. Available at: http://bit.ly/LWmnNR.
Bernstein JA, Bernstein IL, Bucchini L, et al. Clinical and laboratory investigation of allergy to genetically modified foods. Env Health Perspect. 2003;111:1114-21.
Yum HY, Lee SY, Lee KE, Sohn MH, Kim KE. Genetically modified and wild soybeans: an immunologic comparison. Allergy Asthma Proc. 2005;26:210-6.
European Food Safety Authority Panel on Genetically Modified Organisms (GMO). Guidance document for the risk assessment of genetically modified plants and derived food and feed. EFSA J. 2006;99:1–100.
Food and Agriculture Organization (FAO) and World Health Organization. Decision tree approach to the evaluation of the allergenicity of genetically modified foods. In: Evaluation of Allergenicity of Genetically Modified Foods: Report of a Joint FAO/WHO Expert Consultation on Allergenicity of Foods Derived from Biotechnology, 22–25 January 2001. Rome, Italy: Food and Agriculture Organization of the United Nations (FAO); 2001:5–15; 25–27.
Friends of the Earth. Could GM foods cause allergies? A critique of current allergenicity testing in the light of new research on transgenic peas. London, UK; 2006.
Guimaraes V, Drumare MF, Lereclus D, et al. In vitro digestion of Cry1Ab proteins and analysis of the impact on their immunoreactivity. J Agric Food Chem. 2010;58:3222-31. doi:10.1021/jf903189j.
Penninks AH, Knippels LM. Determination of protein allergenicity: studies in rats. Toxicol Lett. 2001;120:171-80.
Pusztai A, Bardocz S, Ewen SWB. Genetically modified foods: Potential human health effects. In: D’Mello JPF, ed. Food Safety: Contaminants and Toxins. Wallingford, Oxon: CABI Publishing; 2003:347–372. Available at: http://www.leopold.iastate.edu/sites/default/files/events/Chapter16.pdf.
Pusztai A. Genetically modified foods: Are they a risk to human/ animal health? Actionbioscience.org. http://www.actionbioscience.org/biotech/pusztai.html. Published June 2001.
American Academy of Environmental Medicine. Genetically modified foods. 2009. Available at: http://www.aaemonline.org/gmopost.html.
Prescott VE, Campbell PM, Moore A, et al. Transgenic expression of bean alpha-amylase inhibitor in peas results in altered structure and immunogenicity. J Agric Food Chem. 2005;53:9023–30. doi:10.1021/jf050594v.
Zolla L, Rinalducci S, Antonioli P, Righetti PG. Proteomics as a complementary tool for identifying unintended side effects occurring in transgenic maize seeds as a result of genetic modifications. J Proteome Res. 2008;7:1850-61. doi:10.1021/pr0705082.
Nordlee JA, Taylor SL, Townsend JA, Thomas LA, Bush RK. Identification of a Brazil-nut allergen in transgenic soybeans. N Engl J Med. 1996;334:688-92. doi:10.1056/NEJM199603143341103.
Originally published at: Earth Open Source[/vc_column_text][/vc_column][/vc_row]
The holiday season is upon us, and parties and family gatherings are happening more often than usual, so I am sharing this infographic that I received from a friend who lost her teenage son to an allergic reaction.
No one wants to be a downer this time of year, but this past year, we saw too many deaths related to food allergic reactions.
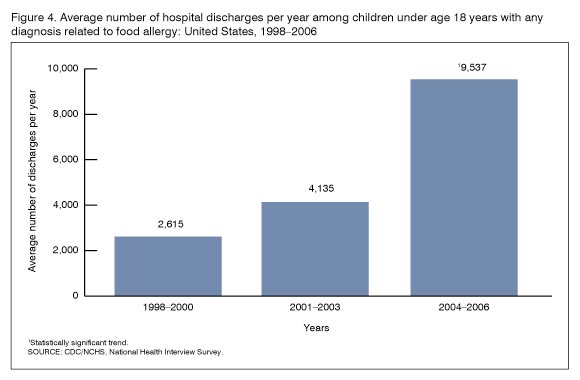
A life-threatening food allergic reaction sends someone to the emergency room once every three minutes in the United States. The EpiPen brand is on fire, hitting $1 billion in revenue because of this condition. It’s serious business, and I truly wish that it didn’t impact as many American families as it does today. From 1997-2007, the rate of hospitalizations related to food allergic reactions increased 265%.
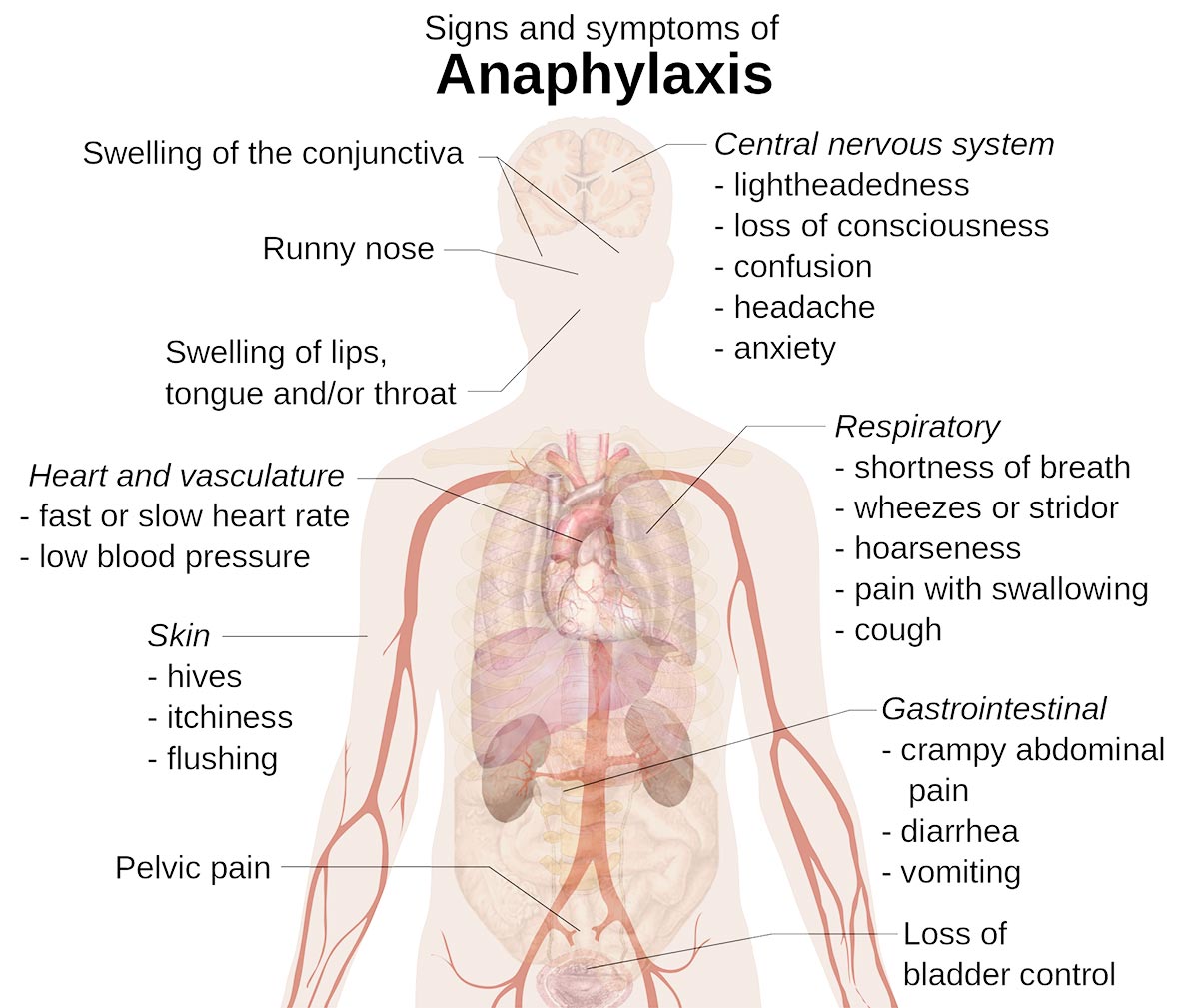
So here is an image that shares the signs of anaphylaxis. Read it through. Share it with your spouse, your children, the people you love. Know the signs.
Recently at the Food Allergy Bloggers Conference, keynote speaker Robyn McCord O’Brien spoke about being the scaffolding for each other as food allergy advocates. Later that day on my panel, AllergyMoms Gina Clowes and attorney Mary Vargas echoed this message. Mary, who is tackling several landmark food allergy cases, pleaded with us to never attack a fellow food allergy advocate online telling us we must always be each others’ support. Take the discussion offline (private message) if you have an issue but don’t be derisive in public because our community needs to be strong and unified. These women are my heroes! But is the message of unity getting to the masses? Based on recent posts directed my way, I fear not.
As far finding a viable treatment for food allergies as I have said in my Huffington Post blogs, this race is not going to be won by astounding sound bytes, but rather by the persistence of analytical research and clinical science. Having said that, I support all those who are participating in both clinical research as well as other avenues of treatment for food allergies. If there are people out there doing TCM (Traditional Chinese Medicine) that are successful, I am so thrilled for them and their families. I have personally supported the efforts of Dr. Li (who I think is phenomenal) and referred many people to her. I am also so happy for those who have participated in Dr. Nadeau’s OIT (Oral Immunotherapy) Study at Stanford, as well as the many others who have found success in various OIT venues. I am truly HAPPY FOR YOU and would never speak poorly of your choice of treatment just because my son is in a different program.
This race is one where we should all be cheering for one another, not trying to break each other’s legs to win the race. What works for your child may not work for mine, and vice versa. Being in a clinical study has given my son a sense of empowerment over his allergy. He feels he is making a difference and can potentially help children just like him. The patch study results are trickling in and so far have certainly been positive. OIT and Chinese herbal therapies have also yielded positive results amongst others. We have no idea which of these many clinical studies will turn out to be the “cure,” but we are proud to participate in the effort to discover it. Please don’t be angry with our family because we are participating in something different than you have chosen.
I invite you to join me in supporting all those in this world who are trying to find solutions and are advocating for those who suffer from life threatening food allergies. Let us support all positive results and efforts, and be each other’s scaffolding in finding a cure.
In peace and love,
Lianne
PS: thank you to the people who are my scaffolding and hold me up in the food allergy world.
The health of our families is changing. With each new diagnosis, whether due to a food allergies, diabetes, a cancer diagnosis or something else, we are learning more about our food and that it now contains a lot of artificial ingredients that aren’t used in other countries.
The journal Pediatrics reports that 15% of American girls are expected to begin puberty by the age of 7 (with the number closer to 25% for African American girls). In the U.S., there is an artificial growth hormone in our milk supply, rbGH, that no other developed country uses. Breyer’s recently dumped this artificial growth hormone, following on the heels of countless other food companies and grocery retailers.
The FDA still hasn’t said much about it.
As I took a look at the FDA’s website on milk, I found something that I hadn’t seen before when it comes to the fortification process where vitamins are added.
For the past almost 20 years, much of our nation’s milk has come from cows injected with a genetically engineered growth hormone.
According to the FDA’s website, “a number of different types of concentrates are available. All contain vitamin D and/or vitamin A palmitate with a carrier consisting of any of the following: butter oil, corn oil, evaporated milk, non-fat dry milk, polysorbate 80, propylene glycol and glycerol monooleate. It is best to store all concentrates under refrigeration unless manufacturer’s directions indicate otherwise. To achieve adequate dispersion, viscous concentrates should be brought to room temperature before addition.”
A growing number of Americans are allergic to milk. Milk allergy has taken the lives of several children. Are we allergic to milk or to what’s been done to it?
Here’s a little history lesson about the introduction of this artificial growth hormones into the American milk supply in 1994.
For the past almost 20 years, much of our nation’s milk has come from cows injected with a genetically engineered growth hormone. If you didn’t know that, you’re not alone. Since it was never labeled, most of us had no idea that this hormone was introduced into our dairy in 1994. The hormone has two interchangeable names: recombinant bovine somatropine (rBST) and recombinant bovine growth hormone (rBGH).
RBGH has dominated the milk market almost since the FDA approved it in 1993. It was the first genetically engineered product ever brought to market. And the Associated Press (AP), the New York Timesand the rest of the media have called it “controversial” (the AP headline actually referred to it as “a bumper crop of controversy”).
So what is rBGH anyway? Although the product is made in a lab, it’s designed to mimic a hormone that’s naturally produced in a cow’s pituitary glands. It’s injected into cows every two weeks to boost their hormonal activity, causing them to produce an additional 10 to 15 percent more milk, or about one extra gallon each day. And within the first four years of its introduction in 1994, about one-third of the nation’s cows were in herds being treated with this growth hormone.
If all you knew about rBGH and this hormone was that it increased milk production, you might think it was a good thing. Why shouldn’t we use every means at our disposal to boost the supply of such a nutritious food?
Well, besides increasing milk production, rBGH apparently does a few other things, too.
First of all, the product seems to be hazardous to the cows. The package itself warns of such bovine problems as “increases in cystic ovaries and disorders of the uterus,” “decreases in gestation length and birthweight of calves,” and “increased risk of clinical mastitis.” Mastitis is a painful type of udder infection that causes cows to pump out bacteria and pus along with milk, requiring treatment with antibiotics and other meds that can end up in the milk.
When I first read this, I had to stop and walk away from the computer for a few minutes. How many bottles and sippy cups had I filled with this milk? Why hadn’t I known about rBGH when I was pouring countless bowls of cereal for my children? I shuddered at the thought that along with the milk, I had also been giving them doses of growth hormone and antibiotics, not to mention potentially exposing them to cow bacteria and udder pus. How had I not known about this Dirty Dairy?
Want some antiobiotics with that growth hormone?
On top of that, and is often cited in the press (most recently by Laurie David), 80% of antibiotics are now used on our livestock here in the U.S. And overexposure to antibiotics tends to kill off the friendly bacteria in our intestines—bacteria that we need for our digestion and immune system. Many doctors believe that too many antibiotics at too early an age is part of the reason that kids are more likely to be allergic: their immune systems aren’t being given the “microbial environment” that they require. Wonder how many “extra” antibiotics our kids are getting in their milk, cheese, and yogurt? Maybe it’s not just about those hand sanitizers.
And then on top of that, allergies are the body’s response to proteins that it considers “toxic invaders,” and that genetically engineered proteins may spark new allergies. According to CNN and a recent study published in the Journal of Allergy and Immunology, milk allergy is now the most common food allergy in the U.S., having risen to the number-one position in the last 10 years. It’s even starting to affect the sale of milk in schools. Might rBGH be a factor in that increase? We wouldn’t have a clue. No human studies were conducted.
The Canadian federal health agency actually found that “the risk of clinical lameness was increased approximately 50 percent” in cows that were given rBGH.
But let’s get back to the cows, because rBGH can hurt them in several more ways. The label also warns of possible increase in digestive disorders, including diarrhea; increased numbers of lacerations on the cows’ hocks (shins); and a higher rate of subclinical mastitis.
Bad enough when dairy cows get visibly sick, because then they’re treated with antibiotics that end up in our milk. But what about the cows who are getting sick at a subclinical level—a level so subtle that farmers don’t notice it? Think of the bacteria and pus pouring out of those inflamed udders—infections that aren’t even being treated! How does drinking that milk affect us, our kids, and our babies in the womb?
Those are just the problems acknowledged on the rBGH product label. Another concern is that the extra hormones drain the cows’ bones of calcium, so that they tend to become lame. The Canadian federal health agency actually found that “the risk of clinical lameness was increased approximately 50 percent” in cows that were given rBGH. Partly as a result, Canada has banned the product, concluding that it “presents a sufficient and unacceptable threat to the safety of dairy cows.”
rBGH is banned in other developed countries but not in the U.S.
Canada isn’t the only country to bar rBGH. The genetically altered hormone has also been banned in the European Union, Japan, Australia, and New Zealand. In addition, the U.N. agency that sets food safety standards, Codex Alimentarius, has refused to approve rGBH not just once but twice.
Farmers themselves have noticed problems with the product. In addition to the expense of the drug itself, rBGH results in higher feed bills, higher vet bills due to increased antibiotic use, and more cows removed from the herd due to illness or low productivity. One study found that 25 to 40 percent of dairy farmers who tried rBGH soon gave it up because it wasn’t profitable enough to justify the damage to their cows. Other farmers have said that they see how hard the product is on cows, and they don’t want to subject their animals to such treatment.
Okay, so that’s why rBGH hurts cows. But I’m way more concerned about us and our kids. How does having a genetically altered hormone in our milk supply affect us?
Health concerns include possible link to cancer
As early as 1998, an article in the Lancet, the prestigious British medical journal, reported that women with even relatively small increases of a hormone known as Insulin-like Growth Factor 1 (IGF-1) were up to seven times more likely to develop premenopausal breast cancer.
And guess what? According to a January 1996 report in the International Journal of Health Services, rBGH milk has up to 10 times the IGF-1 levels of natural milk. More recent studies have put the figure even higher, at something like 20-fold.
Now stop and think about that for a minute, while correlation is not causation, breast cancer used to be something that women got later in life. Premenopausal breast cancer was so rare that when young women presented their physicians with breast cancer symptoms, the doctors often failed to diagnose it, simply because it was so unlikely that an “older women’s disease” would be found among young women.
But according to the Young Survival Coalition, one in 229 women between the ages of 30 and 39 will be diagnosed with breast cancer in the next ten years. Why are all these young women now getting breast cancer? And what about the effects of IGF-1-laden milk on older women, who are already at greater risk for breast cancer?
In case you think that the rising cancer rates have something to do with genetics, stop and think again. According to the Breast Cancer Fund, 1 in 8 women now have breast cancer. But only 10 percent of those cases can be linked to genetics. In other words, 90 percent of breast cancers being diagnosed today are being triggered by factors in our environment.
How did this happen?
Now if you’re like me, your next question probably is, So, if we know all of this, how did this hormone find its way into our dairy products? How did our government agencies, responsible for ensuring the safety of our food, allow the use of this growth hormone and the sale of IGF-1-laden milk? Why was rBGH not used in Europe, Japan, Canada, Australia, and New Zealand, but used so freely right here in our own United States?
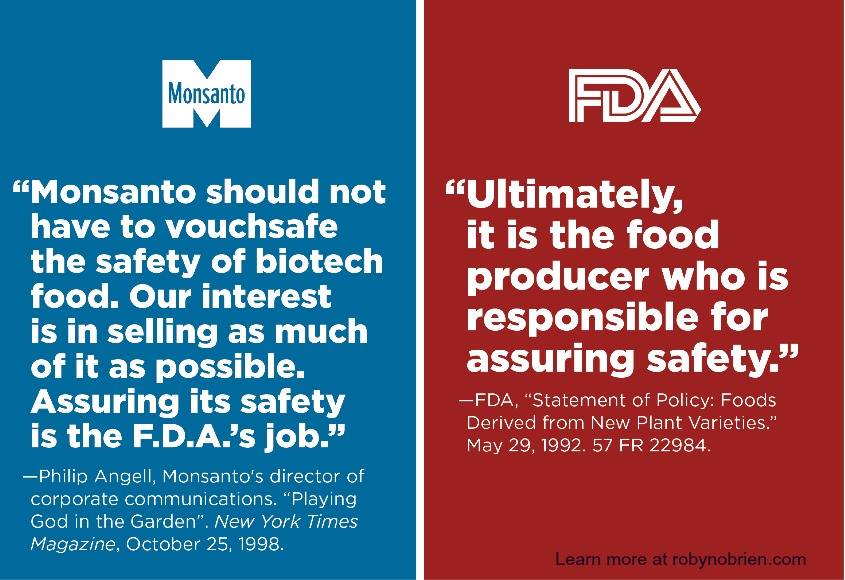
Well, the year before the FDA approved the first genetically engineered protein, it said, “Ultimately, it is the food producer who is responsible for assuring safety.” But at the same time, the corporate communication’s director of Monsanto, company introducing rBGH, said, ” We should not have to vouchsafe the safety of biotech food. Our interest is in selling as much of it as possible. Assuring its safety is the F.D.A.’s job.”
You read that right. It’s kind of a “Who’s on first?” routine. Didn’t we learn anything from the tobacco industry?
So with the jury still out on this one, no long-term human trials ever conducted, a self-regulated industry whose “interest is in selling as much of it as possible,” the increasing rates of antibiotics used on our livestock (not to mention the increasing rates of early puberty and cancer), and the stunning fact that this synthetic growth hormone was never approved for use in Canada, the UK, Australia, New Zealand, Japan and all 27 countries in Europe, maybe it’s time we start to exercise a little bit of precaution here in the U.S., too.
How to Opt-Out of rBGH
Thankfully, we can opt out of this experiment and look for milk labeled “organic” or “rBGH-free”— since by law, these types of milk are not allowed to contain rBGH, a genetically engineered product that was never allowed into the milk, cheese, ice creams and other dairy products in other developed countries. And you can find this milk in Wal-Mart, Costco & Sam’s.
And while correlation is not causation, with the American Cancer Society telling us that 1 in 2 American men and 1 in 3 American women are expected to get cancer in their lifetimes and the Centers for Disease Control reporting that cancer is the leading cause of death by disease in children under the age of 15, a precautionary move like this one just might be what the doctors ordered (at least that’s what they did in all 27 countries in Europe, Australia, Canada, New Zealand, the UK and Japan).
So are we allergic to milk? Or to what’s been done to it?
If you’re new to food allergies, the task of safeguarding your home kitchen can be daunting. With a few straightforward considerations, however, you’ll be ready to cook allergy-friendly meals in no time.
1. Determine the severity of all food allergies in the household. This will help you figure out the degree to which you’ll need to safeguard your house from cross-contamination, according to Cybele Pascal. “If a member of your family is anaphylactic to even airborne traces of peanut, you will be sure to keep peanuts out of the house, and you will do everything in your power to be sure that nothing that’s cross contaminated by peanuts comes into your house. Other families are comfortable having an area of the pantry that is specifically labeled with ‘safe’ foods and utensils for the food allergic person.”
2. Consider a familywide allergy-friendly diet. Some parents find it easier to avoid cross-contamination by eliminating the allergen from the household, especially following the initial food-allergy diagnosis. “With my son, who has multiple food allergies, in the beginning, I just kept all the offending foods out of the house, and we all ate a completely allergy-free diet, which I found was the easiest way of handling it for me,” said Pascal. “Now, we do have some allergens in the house.”[/vc_column_text][/vc_column][vc_column width=”1/3″][vc_empty_space height=”20px”][ultimate_ctation ctaction_background=”#bcbcbc” ctaction_background_hover=”#bfbfbf” text_font_size=”13″]
Featured Food Allergy Experts
Kim Maes is a blogger and the creator of the Cook IT Allergy Free app for iPhone and iPad, which helps food-allergic cooks make safe ingredient substitutions. Her Twitter handle is @CookAllergyFree.
Cybele Pascal is an allergy-friendly chef, blogger and author of two allergen-free cookbooks for food-allergic households. Her Twitter handle is @CybelePascal.
Robyn O’Brien, a former Wall Street food industry analyst, is an author, speaker and founder of the AllergyKids Foundation. Her Twitter handle is @UnhealthyTruth.
[/ultimate_ctation][/vc_column][/vc_row][vc_row][vc_column][vc_empty_space height=”10px”][vc_column_text]3. Stock your kitchen with tools and cooking utensils that are easy to sanitize. The key to a safe kitchen is to minimize your chances for cross-contamination, and the right tools make it easier for you to do so. Both Maes and Pascal advise home cooks to steer away from wood cutting boards and cooking utensils; these items can’t survive the hot diswasher water, and their porous nature can absorb allergens. Instead, opt for plastic cutting boards and silicone or plastic utensils, which are easy to sanitize properly.
Cast-iron cookware is a mainstay in many kitchens; however, Maes points out, “Because these are often meant to be seasoned, particles from previous meals involving allergens can remain on the surface.” In terms of cookware, Maes recommends stainless-steel pans that are dishwasher-safe, such as those from All-Clad, and cast-iron pans dedicated to only allergen-free food. “I leave a label on [the cast-iron pans] when I’m not using them in case someone else is cooking in my kitchen.” Maes’ kitchen also includes dishwasher-safe glass bakeware, stainless cooking utensils, dedicated silicone cooking utensils and a separate labeled toaster for gluten-free bread.
4. Invest in a smart selection of time-saving kitchen gadgets. Since preparing allergy-friendly food may entail a separate cooking process, head to your local kitchen supply store or restaurant supply store for products that can shave off some time. You don’t need to go overboard, however. “Your kitchen needs are no different from a non-food-allergic household,” says Pascal. “Except for the Magic Bullet, perhaps. This is a great way to make shakes for my food-allergic son.” Pascal also swears by her microplane, her mixing bowls from Crate and Barrel, and her Kitchen Aid stand mixer.
Avoiding Cross-Contamination
A well-stocked kitchen isn’t enough to safeguard your family from foods that could trigger an allergic reaction. You’ll also need to study up on cross-contamination, which may mean relearning several aspects of cooking at home.
5. Sanitize your hands, thoroughly and often. “I can’t stress how important this step is,” says Pascal. “Wash your hands between each step while prepping and cooking, with warm water and soap, and dry them on a clean paper towel or fresh dish towel.”
6. Clean and sanitize food-preparation areas before, during and after the cooking process. “Wash down kitchen surfaces. Don’t just wipe or brush them off — clean them thoroughly. I’m talking counters, cabinet knobs, the faucet and the surface of that salt shaker,” Pascal says. “Be sure that all equipment, pans and utensils have been thoroughly washed and sanitized before you use them.”
7. Assign dedicated “safe” shelves in your kitchen cabinet, pantry and refrigerator. “I separate shelves in my pantry and in my refrigerator to designate which foods are allergen-friendly and safe for the food-allergic family members,” says Maes. “This [method] is great for caregivers who may not be aware what is safe for your children to eat.”
8. Also assign dedicated “safe” kitchen appliances and utensils. Pascal recommends using separate cutting boards, with at least one that’s designated for preparing allergy-free meals. “You may also wish to have separate pans and utensils,” she adds. “More expensive, but less risky. Be sure to label them and keep them in a separate area when they’re not in use.” Pascal also advises parents to label and separate eating utensils for food-allergic individuals.
9. For households with wheat allergy or celiac disease, purchase a separate toaster for gluten-free bread. “If you use the same toaster for both gluten-filled and gluten-free bread, you are at a great risk for contamination,” warns Maes. Both Maes and Pascal recommend a separate toaster for gluten-free bread; if you don’t have the space or budget, Maes notes that the safest alternative is to place gluten-free bread on a piece of foil during toasting to avoid contact with gluten particles.
10. Time and prepare your meals so that the allergic person’s food is completed first. “Prepare the food-allergic person’s food first, and then cover it and set it aside to be sure nothing migrates into it. Serve the food-allergic person first to avoid cross-contamination from serving utensils,” says Pascal.
11. Educate the whole family on sanitation best practices. If you choose to have food allergens in your home, make sure your whole household remains vigilant on keeping “safe” items free of allergens. “If you have an egg allergy and someone dips his or her knife into the mayonnaise and then follows it up by dipping into the mustard, the mustard has now been contaminated with egg particles for any future uses,” warns Maes. The same goes for making peanut butter and jelly sandwiches, spreading jam on a piece of toast, or using any other condiment in the kitchen. “These minute amounts might seem insignificant; however, for someone with a life-threatening food allergy, they could spell disaster.”
Ensuring a Balanced Diet
12. Embrace whole, fresh foods. Since food-allergic individuals must cut so many foods out of their repertoire, many parents worry about proper nutrition and a balanced diet. Robyn O’Brien has a simple mantra to help: Eat Less Fake Food. Here’s O’Brien’s rationale behind this mantra:
We were feeding our kids blue yogurt, chicken nuggets, and mac and cheese when we first found out that our fourth child had food allergies. And then to learn that processed foods contain new allergens and proteins (not found in kids’ foods in other developed countries) that aren’t listed on the labels — what mom has time for that? So we decided to try to Eat Less Fake Food. And it goes such a long way in reducing your children’s exposure to hidden allergens, chemicals and preservatives now in the food supply that weren’t there when we were kids. Since 70 percent of a child’s immune system is found in his digestive tract, by simply eating less fake food, you are doing so much to ensure the health of a child and not corrode those digestive pipes with food pumped full of chemicals.
The number of people in the U.S. with food allergies is skyrocketing.
The rate of people with peanut allergy in the United States more than quadrupled between 1997 and 2010. A life-threatening food allergic reaction now sends someone to the E.R. once every three minutes in the U.S.
The food industry is getting in on it. Mondelez, formerly known as Kraft, recently acquired Enjoy Life Foods, a popular and well-loved brand in the allergy space, free from many of the top eight allergens and also free from genetically modified ingredients.
It was a $40 million company that was acquired for $130 million.
What does Mondelez plan to do with the acquisition? Grow it into a billion dollar brand.
What are some other billion dollar brands? Cheerios, Lays, Pepsi, Starbucks….
And EpiPen.
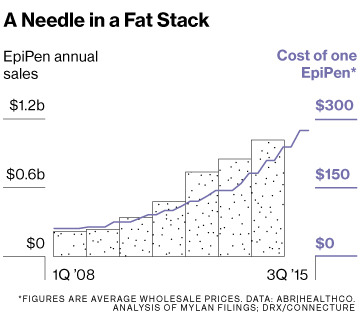
According to Bloomberg, “In a 2007 purchase of medicines from Merck, drug maker Mylan picked up a decades-old product, the EpiPen auto injector for food allergy and bee-sting emergencies. Management first thought to divest the aging device, which logged only $200 million in revenue. Today, it’s a $1 billion-a-year product that clobbers its rivals and provides about 40 percent of Mylan’s operating profits.”
Food allergies are not a niche, it is a growing epidemic that is challenging how we think about our food and how it is made. Genetic factors don’t change this quickly, environmental factors do. Are we allergic to food or to what’s been done to it? The biotech industry will say there is no evidence of any harm from genetically engineered foods. Since we didn’t label these foods in the U.S., there is no evidence period. But what if we had labels? We would have more data.
Someone who has a horrific reaction to e.coli in organic spinach can trace it back to the organic spinach, because it is labeled. Genetically engineered ingredients aren’t labeled in the U.S. Because these ingredients are not labeled, there is no traceability, and with that, no accountability and no liability should these ingredients prove to cause harm.
But it doesn’t stop allergic reactions from happening, so a lot of families have to pay more for free-from food.
Researchers report that the costs of food allergies, from medical care to food to pharmaceuticals is $4,184 per child per year, costing our economy $25 billion, including lost productivity.
Researchers reporting in the Journal of the American Medical Association states that the costs of food allergies, from medical care to food to pharmaceuticals is $4,184 per child per year, costing our economy $25 billion, including lost productivity.
On top of that, the costs to families with food allergies is skyrocketing. After insurance company discounts, a package of two EpiPens costs about $415. By comparison, in France, where Meda sells the drug, two EpiPens cost about $85. Back in 2007, when the company was purchased, it cost $57. EpiPens wholesale price rose 400% since 2007 and 32% in the last year alone. EpiPen margins were 55 percent in 2014, up from 9 percent in 2008.
According to Bloomberg, the company’s marketing techniques play on the fears of parents and caregivers. There is no incentive here to find a cure or to stop the condition. Sales are explosive.
To discount this condition in any way is irresponsible, but it is just one of the conditions that is triggering a food awakening around the country.
In the last year, Target, Chipotle, Kroger, even General Mills and Cheerios have responded to this growing demand in the marketplace. Free-from foods are showing up in Dollar Tree stores.
These companies aren’t stupid. They see the escalating rates of diseases in their own employees, they feel the financial impact with their own health care costs, and they hear consumers that are saying they want to eat fewer fake, artificial and genetically engineered ingredients.
While the chemical companies selling these new ingredients say there is no evidence of harm, consumers are saying: there is no evidence since these ingredients were never labeled in the United States.
In other words, if you walked into an allergist’s office and asked if you were allergic to soy that has been in the food supply for thousands of years or if you are allergic to Roundup Ready soy, non-GMO soy treated with Roundup or organic soy, there would be no test to give you that answer. Next time, you are at the allergist’s office, ask which soy they are testing for.
With no labels on GMO ingredients in the US to trace their impact and no test to offer definitive answers, the biotech industry is able to claim that there is not a single documented case of these foods ever causing harm.
Not sure what the explosion in EpiPen sales says. But it’s significant. It’s significant to the families that use them and delivers significant revenue to the pharmaceutical company selling them, especially here in the United States.
A study released in the Journal of the American Medical Association, says yes, living in the United States increases your risk of allergic diseases……“significantly.”
“Living in the US raises risk of allergies,” says the headline.
According to the research, living in the United States for a decade or more may raise the risk of some allergies, reports the Journal of the American Medical Association.
“These data indicate that duration of residence in the United States is a previously unrecognized factor in the epidemiology of atopic disease,” it said.
In other words, the longer you live here, the more likely you are to develop some kind of allergy, asthma, eczema or other related condition.
Food allergies have been skyrocketing in the United States in the last fifteen years. Not only has the CDC reported a 265% increase in the rates of hospitalizations related to food allergic reactions in a ten year period, but the sales of EpiPens, a life-saving medical device for those with food allergies, has also seen record sales growth according to the New York Times.
So what’s going on?
The study aimed to find out. Allergies reported in the survey included asthma, eczema, hay fever, and food allergies.
“Children born outside the United States had significantly lower prevalence of any allergic diseases (20.3%) than those born in the United States (34.5%),” said the study led by Jonathan Silverberg of St. Luke’s-Roosevelt Hospital Center in New York.
Let’s restate that:
Children born in the US have more than a 1 in 3 chance of having allergic diseases like food allergies, asthma or eczema, while kids born in other countries around the world had a “significantly lower prevalence” of 1 in 5.
On top of that, “foreign-born Americans develop increased risk for allergic disease with prolonged residence in the United States,” it said.
In other words, if you move here, your chances of developing any one or more of these allergic diseases increase.
The study went so far as to say that children born outside of the US who moved here showed “significantly” higher odds of developing these diseases.
What’s driving this? Is it really Purel and intense handwashing? And the hygiene hypothesis?
And are we allergic to food? Or what’s been done to it?
Because genetics don’t change that quickly, and the environment does.
This presents a risk not only to these children, but also to our economy, as the financial burden of these conditions and their associated health care costs impact not only families but also our country, our military and our productivity.
So what is triggering this escalating, US allergy epidemic?
According to Reuters report on the study and Dr. Ruchi Gupta, who studies allergies at the Northwestern University Feinberg School of Medicine in Chicago but wasn’t involved in the new research, “This is definitely something we see clinically and we’re trying to better understand, what is it in our environment that’s increasing the risk of allergic disease?” said
“Food allergies have increased tremendously,” she told Reuters Health. “We do see people who come from other countries don’t tend to have it.”
Genetically engineered crops are created by inserting a protein from a different organism into the original crop’s genome. This is usually done to create a plant that is more resistant to insects or diseases.
The Food and Agriculture Organization within the World Health Organization has a structured approach to determining whether genetically engineered foods cause allergies, according to Venu Gangur, MSU assistant professor of food science and human nutrition, who also is a faculty member in the National Food Safety and Toxicology Center. “But it has a major flaw. A critical question in that process asks, ‘Does the protein cause an allergic reaction in animals?’ The problem is that there has been no good animal model available to test this.”
It’s food for thought.
The cost of food allergies is burdening more than just the families dealing with them, it’s burdening our schools, our health care system and our economy. It has become a billion dollar business in less than a decade for the company making EpiPens.
Just as cancer isn’t a niche, food allergies are no longer a fad.
In the U.S., food allergies now affect 1 in 13 children. Food allergies send someone to the E.R. once every three minutes.
Last year, one mom decided to paint a pumpkin teal blue to say that her house would be a safe house for kids with food allergies to trick or treat. It went viral, and this display is from a Hy-Vee in Illinois for this year.
The image on the left is from Safeway this year, a sign most likely developed by the Tootsie Roll company.
Food allergies are real and escalating. A growing number of Americans, not just children, are impacted.
Thankfully, grocery stores understand.
From 1997-2007, the CDC reported a 265% increase in the rates of hospitalizations related to food allergic reactions. The rate of the peanut allergy quadrupled from 1997-2010.
Are we allergic to food or to what’s been done to it?
Please share this post and this image. Spread the word.
In memory of Emily, Gio, Sara and so many others who have lost their lives to a food allergic reaction.
Today, a food allergic reaction sends someone to the emergency room once every three minutes in the United States. According to the CDC, there was a 265% increase in the rate of hospitalizations related to food allergic reactions between 1997 and 2007. 1 in 13 children in the U.S. now has a food allergy, and as many as 50 million Americans are allergic to something.
More people have food allergies than ever before, airlines are considering carrying EpiPens, a life-saving device and injection of epinephrine on flights, so knowing what to do in case of a severe allergic reaction could help save a loved one’s life.
Sometimes, food allergies are diagnosed early, and sometimes the diagnosis comes when a life-threatening allergic reaction occurs.
This short video shows what to do in an emergency. Please share this with family, friends, your school, church and community. It just might save a life.
I’ve heard that there’s no style of learning more effective than experiential learning. This stands to reason. Here are some things I’ve thought and some things I’ve learned through experience.
I’ve thought, “What a freaking nuisance. You know this is just an overprotective helicopter mom and because of her, because of these two or three nut jobs, I can’t make myself a damn peanut butter sandwich without breaking building ordinances. Anywhere.”
I’ve thought, “Don’t worry about it. We’ve got it covered. Sure, little Billy’s mama made a stink about it, but we got one of the pizzas with soy cheese. We’re not jerks, of course we want the kid to be safe and able to have fun.
I’ve thought, “This is the mom’s issue.” “The poor kid gets stuck at the table with all the other kids he doesn’t know and has to have a special plate of crap brought out to him with his name on it. All because mom loves the attention she gets calling 13 times a day to make sure he’s not eating anything other than what is on the stupid list.”
I’ve thought, “Seriously, what’s the worst that could happen?”
I’ve rolled my eyes and used air quotes when explaining that a kid in my care, but not my kid, had “food allergies” and gone on to explain — in coded, but witheringly judgmental, language — said child’s mom and her hyper anxiety.
Whether it was coincidence or not, it was always the moms.
Thank God, none of these misconceptions had fatal outcomes or even critical ones.
Then experience came knocking and taught me in an afternoon how mistaken I was.
Do you remember your 9/11 story? I do. For years after that terrible day, anytime you were with someone you either didn’t know before or hadn’t seen since before that tragic day the conversation always got around to your story. Your experience of that day. It still happens, just not as much, as more and more “adults” are not of an age to have remembered it, or you’re so familiar with everyone’s tales that you reference rather than recount them.
Parents of kids with anaphylactic food allergies engage in the telling and retelling of our tales whenever we find someone that gets it. Unfortunately for us and our kids, parents of kids with anaphylactic food allergies are the only ones that get it. Each of us encounters the “me” from above, who doesn’t get it, and we know they don’t get it and that only makes us act crazier.
See, we have to be crazy. So crazy that you’d rather just bitch about me and my hyper anxiety then have to deal with my crazy wrath if any of my seemingly bizarre and self-centered requests are found to have been ignored. We’ve been granted the greatest education possible through our experiences. Here’s what I’ve learned.
Many parents have a crazy period early in their first child’s life, often during the first week or two, when they can’t stop thinking that it’s possible the baby will stop breathing and just die. We had this bit of experiential learning ourselves, and for a 10-day period after getting the kid home, one of us was awake at all hours of the day and night to make sure this didn’t happen.
How we’d stop it if it did is something we never even considered. It just seemed like the right thing to do. Then we realized that was crazy; if he was going to give us a few minutes we needed to take them. Parents learn those fears are baseless.
A year or so later, we were having our normal lunch. Then little red pinpricks appeared around our son’s red and watering eyes. That’s weird. Then bright red blotches all over his face and a high whistle from the air trying to get in and out. Then running to the car. Then heavy vomiting, as it was the only way it seemed he could get breath. Then, no breathing and beet red. Then enormous vomiting.
Do you know where you park at the ER if your 1-year-old baby is red and unable to breathe, turning purple, and you and your wife and your baby are covered in vomit as he writhes to try to loosen the vice grip of the snake he feels choking him, only it’s not a snake, it’s his own body choking him from the inside?
Wherever the fuck you want.
In our case it was at the door. The car was vomit-filled, and I mean vomit was covering the windows, all of them, including the windshield. By “at the door,” I mean they saw us and guided us right to the door. We left our car there, running, doors open.
Until that day, my experience at the ER had never failed to include a stop for at least a second of triage. Not this time. They saw the baby, saw he was barely holding on to his precious little life and the breaths were gone, and they pointed and told us “RUN!!” and we did. Adrenaline was flooding our bodies and brains and we did it. We ran.
When we got there we didn’t care who was there. We just needed someone to save our baby’s life. They did. We calmed down on the outside and panicked on the inside.
Eventually he was laughing and playing and my wife and I were trying to reflect his carefree demeanor, sneaking in conversation about what the hell it could be. We wouldn’t get answers until we saw the allergist a few days later. So we emptied our kitchen. Almost all of it. Because something in there could cause that silly fear we had as new parents to become a reality. Our little love could just die. It’s knowledge we will carry until there is either a cure or we die.
That’s it. That’s the list of all the ways we came to stop worrying. We got better at living with the knowledge, but we reordered everything, including our priorities.
I used to have a career working in the city, but since I know from all my conversations how many people think this whole “food allergy thing” is being way overblown by nervous parents, I ignored that job and rested on the laurels I’d earned. Once those were used up, I relied on the sheer audacity to just show up late, leave early or not show up at all, while trying to find something that worked closer to home, since we were told that if he went into shock the staff at the daycare couldn’t go with him; he would just be taken by the ambulance, terrified, waiting, perhaps for hours, until we arrive.
So, I took a $20,000 pay cut and took a gig, a good gig, one I love, but a step down to be sure, to be with him for the day, feet away, always ready to run. I’ve done it once and hope to never do again.